

What if the biggest movie conflicts of all time could be fixed with one sensible choice? This...
Thirdhand smoke is the toxic tobacco residue that clings to walls, carpets, furniture, clothing, cars, dust, skin,...
What changes when guests attend more than one wedding for the same person? More than you might...
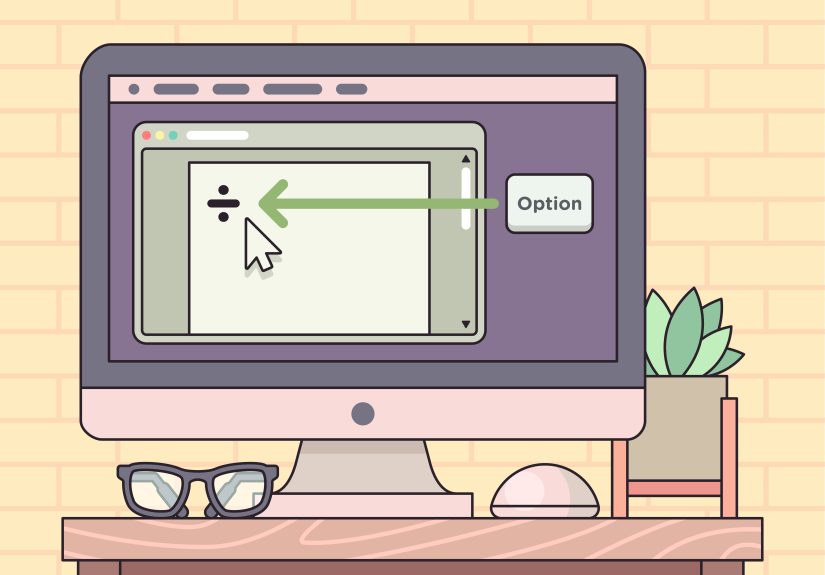
Need to type the division symbol but cannot find it on your keyboard? This clear, friendly guide...
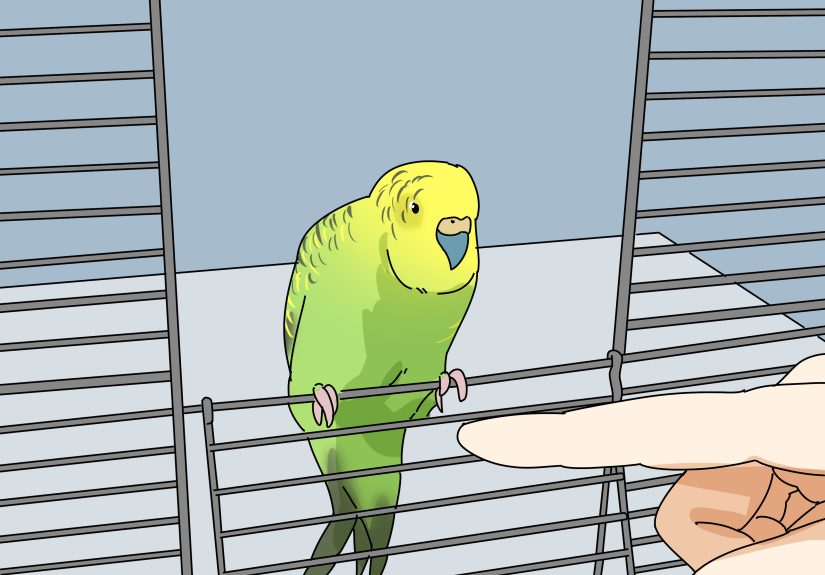
Got a budgie with strong opinions and a sharper beak than expected? This in-depth guide explains how...

Greenland’s so-called zombie ice is not science fiction. It is doomed ice already committed to melting, and...

What is your why? It is the deeper reason behind your choices, goals, relationships, and daily habits....

Need a deity name that sounds ancient, powerful, and unforgettable? This God Name Generator guide shows you...

Skin pH sounds technical, but it affects how your skin looks, feels, and functions every day. This...

What happens when American medicine meets Roman life? This in-depth guide explores the reality of being an...