




Strontium gets a lot of attention in osteoporosis conversations, but the truth is more complicated than supplement...
Who is Erica Cheah? This in-depth profile explores the Canada-based media leader and photographer whose public career...
A sore throat and stiff neck can show up together for several reasons, from common viral infections...
Business crime insurance helps protect companies from direct financial losses caused by employee theft, forgery, robbery, computer...
The Open Globe Shade - Opal is more than a simple glass shade. It softens glare, adds...

Want your credit card points to work harder? This in-depth guide explains how Star Alliance, oneworld, and...
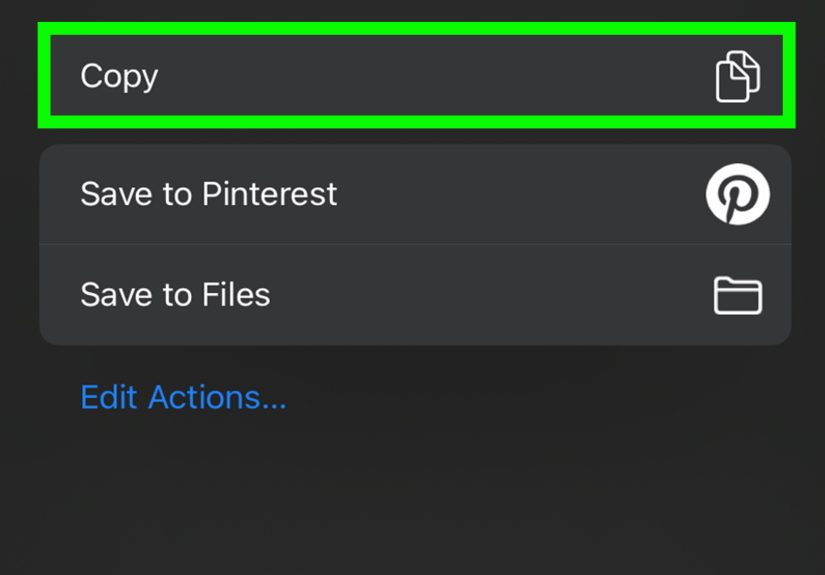
Need to copy text, links, or details from an email on your iPhone or iPad without the...

Shopping for the best robot vacuum in 2025? This in-depth guide breaks down BHG’s top-tested picks for...

Looking for fun, low-stress ways to get creative? These 6 easy DIY art projects are perfect for...

The Falcon Enamelware Teapot is more than a pretty countertop piece. This in-depth guide explores its heritage,...