Table of Contents >> Show >> Hide
- Fibroids 101: The Quick, Useful Version
- What the Numbers Say: How Common Are Fibroids in Black Women?
- So… Why the Disparity? It’s Not One ThingIt’s Many Levers Pulling at Once
- 1) Genetics and family history: some risk is inherited
- 2) Hormone sensitivity and growth signals: same hormones, different response
- 3) Vitamin D deficiency: a clue that keeps showing up
- 4) Hypertension and metabolic factors: blood pressure matters
- 5) Earlier puberty/menarche: more years of cycling, more years of exposure
- 6) Environmental exposures: endocrine disruptors and the “personal care product” hypothesis
- 7) Chronic stress and structural racism: biology carries what life hands it
- 8) Diagnosis and treatment inequities: when care arrives late, disease looks worse
- Symptoms You Should Never Be Told to “Just Live With”
- How Fibroids Are Diagnosed
- Treatment Options: From “Let’s Monitor” to “Let’s Fix This”
- How to Advocate for Yourself (Without Needing a Law Degree)
- Can Fibroids Be Prevented?
- Bottom Line
- Experiences People Commonly Share (Especially Black Women Navigating Fibroids)
- SEO Tags
If your period has ever shown up like it’s moving apartmentsbringing heavy bleeding, big cramps, and a schedule that refuses to respect your calendaryou’re not alone. Uterine fibroids (also called uterine leiomyomas) are one of the most common gynecologic conditions in the United States. They’re noncancerous growths made of uterine muscle tissue, and they can range from “tiny and quiet” to “how is my uterus doing this?”
Here’s the part that deserves a spotlight: Black women are more likely to develop fibroids, tend to develop them younger, and often experience more severe symptoms than other groups. That’s not because Black bodies are “built wrong,” and it’s not because anyone did something to “cause” them. It’s because fibroids are shaped by a messy intersection of biology, environment, and health-system realitiesand in the U.S., those factors don’t fall evenly across communities.
This article breaks down what we know (and what we’re still figuring out), why the disparity exists, and how to advocate for good care if fibroids are affecting your life.
Fibroids 101: The Quick, Useful Version
Uterine fibroids are benign growths that form in or on the uterus. They can be single or multiple, and they may grow slowly, quickly, or not at all. Some people never notice them; others can’t ignore them if they tried.
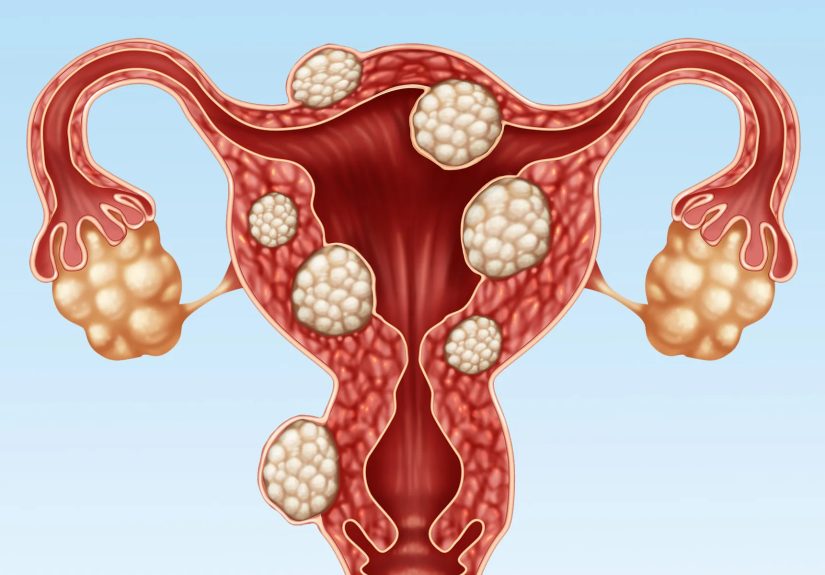
Common fibroid locations (and why they matter)
- Intramural fibroids: within the uterine wall (often linked with heavy bleeding and bulk symptoms).
- Submucosal fibroids: bulging into the uterine cavity (often the biggest troublemakers for heavy menstrual bleeding).
- Subserosal fibroids: on the outer surface of the uterus (more likely to cause pressure symptoms).
Symptoms fibroids can cause
- Heavy menstrual bleeding or long periods
- Iron-deficiency anemia (fatigue, dizziness, shortness of breath)
- Pelvic pressure, bloating, or “always feeling full”
- Frequent urination or trouble emptying the bladder
- Constipation or rectal pressure
- Pelvic pain, cramps, or pain during sex
- Fertility and pregnancy challenges (depending on size/location)
Fibroids are often described as “estrogen- and progesterone-responsive,” meaning they tend to grow during reproductive years and may shrink after menopause. But “tend to” is doing a lot of work therebecause individual experiences vary wildly.
What the Numbers Say: How Common Are Fibroids in Black Women?
Fibroids are common in general. What’s different is the timing and burden. Large U.S. studies using ultrasound screening (which catches fibroids that haven’t been diagnosed yet) have found that by about age 50, an estimated more than 80% of Black women and roughly about 70% of White women have developed fibroids. In other words: many people will have them, but Black women are more likely to develop them earlier and often with greater symptom impact.
Black women are also more likely to have:
- Earlier onset (fibroids appearing at younger ages)
- More numerous or larger fibroids
- More severe symptoms, especially heavy bleeding and pain
- Higher rates of fibroid-related proceduresincluding major surgeries
And there’s another layer: fibroids can be underdiagnosed for years, especially when heavy bleeding is dismissed as “normal,” pain is minimized, or people are told to just “tough it out.” When diagnosis is delayed, fibroids have more time to grow and cause complications.
So… Why the Disparity? It’s Not One ThingIt’s Many Levers Pulling at Once
If you’re looking for a single villainone gene, one product, one food, one hormonefibroids will disappoint you. The most accurate explanation is also the least satisfying: fibroid risk is influenced by multiple factors, and in the U.S., several of those risk factors occur more often (or hit harder) in Black women due to a combination of inherited biology, lived environment, and structural inequities.
Here are the biggest contributors researchers talk about, in plain English.
1) Genetics and family history: some risk is inherited
Fibroids often run in families. If your mother or sister had fibroids, your risk is higher. Researchers also know that fibroids can contain specific genetic changes in the tumor tissue itself, which helps explain why fibroid cells behave differently from normal uterine muscle cells.
That said, genetics alone doesn’t explain the full racial disparitybecause genes don’t change fast, but fibroid burden can shift with environment, stress, and access to care. Think of genetics as the “loaded playlist,” not the “press play button.”
2) Hormone sensitivity and growth signals: same hormones, different response
Fibroids are influenced by estrogen and progesterone, but hormones don’t act in a vacuum. They interact with growth factors, inflammation pathways, and tissue responses that may vary from person to person. Some research suggests that differences in how fibroid tissue responds to hormonal signals may contribute to severity patterns seen in Black women.
Translation: it’s not just how much hormone you haveit’s how your uterine tissue responds to it over time.
3) Vitamin D deficiency: a clue that keeps showing up
Vitamin D is famous for bones, but it also plays roles in immune regulation and cell growth. Multiple studies have found associations between lower vitamin D levels and a higher likelihood of fibroids or greater fibroid burden.
In the U.S., vitamin D deficiency is more common in Black individuals in part because higher melanin levels reduce vitamin D production from sunlight, and because broader health and environmental factors influence diet, supplementation, and outdoor exposure. This doesn’t mean vitamin D is the magic switch that “causes” fibroidsbut it is a meaningful, potentially modifiable piece of the puzzle.
Practical takeaway: If you have heavy bleeding or known fibroids, ask a clinician whether checking vitamin D and iron levels makes sense for you. (And don’t mega-dose supplements without medical guidancemore isn’t always better.)
4) Hypertension and metabolic factors: blood pressure matters
High blood pressure has been repeatedly linked with fibroid risk. Recent large studies suggest that people with untreated or newly developed hypertension may have a higher risk of being diagnosed with fibroids, while treatment and control of blood pressure may be associated with lower risk.
Why would blood pressure connect to uterine growths? Researchers suspect shared pathways involving inflammation, blood vessel function, and tissue remodeling. And because Black women in the U.S. are disproportionately affected by hypertension (driven by many social, environmental, and access factors), this may contribute to the fibroid burden as well.
Body weight can also play a role. Adipose (fat) tissue influences hormone metabolism and inflammation. Again: this is not about blameit’s about biology interacting with lived realities, including food environments, stress, sleep, and healthcare access.
5) Earlier puberty/menarche: more years of cycling, more years of exposure
Earlier age at first period (menarche) has been associated with higher fibroid risk and, in some studies, with more severe fibroid outcomes. One common explanation is cumulative exposure: the earlier menstrual cycles begin, the longer uterine tissue is exposed to cyclic hormonal signaling across decades.
Some U.S. data show that Black girls, on average, experience puberty earlier than some other groupslikely due to a mix of genetics, environment, nutrition, stress, and endocrine-disrupting exposures. More years of cycling may be one more lever nudging fibroid risk upward.
6) Environmental exposures: endocrine disruptors and the “personal care product” hypothesis
Endocrine-disrupting chemicals (EDCs)like certain phthalates and parabenscan interact with hormone pathways. Research is exploring whether these exposures contribute to fibroid development or growth.
This matters for Black women because exposure patterns can differ based on marketing, product availability, and cultural beauty norms. Some recent studies have examined hair product use (including straighteners, relaxers, and dyes) and fibroid outcomes specifically in Black populations. The evidence is still evolving: associations don’t always mean causation, and products/formulations vary over time. But it’s an active area of research, and it’s one reason many experts now talk about fibroids through an “environment + hormones + tissue response” lens.
Practical takeaway: If you want a low-stress way to reduce potential exposure, consider:
fragrance-free options when possible, limiting products with “parfum,” and choosing brands that disclose “phthalate-free” or “paraben-free” claims. This won’t guarantee fibroid preventionbut it can reduce endocrine-disruptor exposure overall.
7) Chronic stress and structural racism: biology carries what life hands it
Chronic stress affects cortisol, inflammation, sleep, immune function, and metabolic healthall systems that can influence reproductive health. Importantly, research has found that perceived racial discrimination has been associated with increased fibroid risk in Black women in the U.S.
This is not about “stress causing fibroids” in a simplistic way. It’s about long-term wear-and-tear (sometimes described as allostatic load) affecting the body’s regulatory systems. When stress is tied to racism and socioeconomic inequity, it becomes a public health issuenot a personal failing.
8) Diagnosis and treatment inequities: when care arrives late, disease looks worse
Black women often face barriers to timely diagnosis and a full range of treatment options. That can include:
insurance gaps, fewer specialist options nearby, long wait times, dismissal of symptoms, and fewer chances to try less invasive treatments early.
When fibroids are finally addressed after years of heavy bleeding or pain, they may be larger or more numerousmaking major surgery more likely. This is one reason experts emphasize culturally competent care and shared decision-making, especially around fertility goals and uterus-sparing options.
Symptoms You Should Never Be Told to “Just Live With”
Some discomfort during a period is common. “Common,” however, is not the same as “fine.” Consider getting evaluated if you have:
- Bleeding that soaks through a pad or tampon in an hour (especially for several hours)
- Periods that routinely last longer than 7 days
- Clots larger than a quarter
- Fatigue, dizziness, or shortness of breath (possible anemia)
- Pelvic pressure, frequent urination, constipation, or pain with sex
- Trouble getting pregnant, recurrent pregnancy loss, or pregnancy complications
If anyone tells you “that’s just what periods are like,” you have permission to mentally file that under: Incorrect, next.
How Fibroids Are Diagnosed
There’s no routine fibroid screening program for everyone. Most diagnoses happen when symptoms show up or when imaging is done for another reason. A typical workup may include:
- Health history + pelvic exam
- Ultrasound (often the first-line imaging test)
- Blood tests if heavy bleeding suggests anemia (iron studies may be included)
- MRI in select cases to map fibroids more precisely before certain procedures
Good care also means making sure heavy bleeding isn’t being caused by something else. Fibroids are common, but they’re not the only explanation.
Treatment Options: From “Let’s Monitor” to “Let’s Fix This”
Fibroid treatment should match three things: symptoms, fibroid location/size, and your life plans (especially fertility goals). You deserve to hear more than one option.
Medication options (symptom control and short-term shrinkage)
- NSAIDs (like ibuprofen) for cramps and some bleeding reduction
- Tranexamic acid for heavy menstrual bleeding (taken during heavy days)
- Hormonal contraceptives (pills, patch, ring) to manage bleeding patterns
- Levonorgestrel IUD (in some cases) to reduce heavy bleeding
- GnRH agonists (temporary “medical menopause,” sometimes used pre-surgery)
- GnRH antagonists with add-back therapy to treat heavy bleeding for a limited duration (often up to 24 months, depending on the medication and guidance)
- Iron supplementation if anemia is present (paired with treating the bleeding source)
Medications often improve symptoms but may not permanently eliminate fibroids. Still, symptom relief can be life-changingespecially when it helps you avoid anemia, miss fewer workdays, or get through the month without planning your wardrobe around “just in case.”
Procedures and surgeries (target the fibroids more directly)
- Myomectomy: removes fibroids while preserving the uterus (often preferred if pregnancy is a goal)
- Uterine artery embolization (UAE/UFE): blocks blood flow to fibroids so they shrink (not always ideal if future fertility is a priority)
- Radiofrequency ablation: uses heat to shrink/destroy fibroid tissue (fertility considerations vary)
- MRI-guided focused ultrasound: noninvasive approach for select cases
- Hysterectomy: removes the uterus (definitive cure for fibroids; ends fertility)
If you want children now or later, say that early in the conversation. Some treatments can affect fertility, pregnancy outcomes, or future uterine structure. A good clinician won’t just hear your symptomsthey’ll hear your goals.
How to Advocate for Yourself (Without Needing a Law Degree)
Because fibroids can be dismissed or minimized, it helps to come prepared. Consider asking:
- Where are my fibroids located (submucosal, intramural, subserosal)? How many? How big?
- Are my symptoms consistent with fibroids, or do we need to rule out other causes of bleeding?
- Am I anemic? Should we check ferritin and iron levels?
- What are my uterus-sparing options?
- What are the pros/cons of medication vs procedure vs surgery for my situation?
- If I want pregnancy, which options best protect fertility?
- What happens if we do nothing for 6–12 months?
And if you feel brushed off, it’s okay to say: “I’d like to understand all my options, including less invasive ones.” That sentence is polite, firm, and extremely hard to argue with.
Can Fibroids Be Prevented?
There’s no guaranteed way to prevent fibroids. But because risk is influenced by multiple factors, some steps may help lower overall risk or reduce symptom burden:
- Manage blood pressure with regular monitoring and treatment if needed
- Address vitamin D deficiency if present (with clinician guidance)
- Maintain iron stores and treat anemia early
- Prioritize sleep and stress reduction (not as “self-care fluff,” but as body regulation)
- Reduce endocrine-disruptor exposure where practical (fragrance-free, ingredient-aware choices)
- Seek evaluation early when bleeding/pain changesearlier care can mean more options
Most importantly: fibroids are common, treatable, and worthy of attention. You don’t need to “earn” medical care by suffering long enough.
Bottom Line
Uterine fibroids are particularly common in Black women because the drivers of fibroid riskgenetics, hormone responsiveness, vitamin D deficiency, hypertension, environmental exposures, chronic stress, and healthcare inequitiesstack in ways that disproportionately affect Black women in the U.S. The disparity is real. The suffering is real. And the solutions require both good medical care and better systems.
If you take one thing from this article, let it be this: heavy bleeding and chronic pelvic pain are not personality traits. They’re symptoms. And you deserve answers and options.
Experiences People Commonly Share (Especially Black Women Navigating Fibroids)
Data explains the “what,” but lived experience explains the “why this is so exhausting.” Below are themes that come up again and again in patient stories, support groups, and clinic conversationsespecially among Black women, who often carry a double burden: more severe fibroids and more barriers to care.
“I thought this was normal… because everyone told me it was.”
One of the most common experiences starts with normalization. A teenager gets heavy periods early, adults call it “just part of being a woman,” and the message sinks in: bleeding through products, missing school, and curling up with cramps is simply the cost of admission. Years later, the person is planning life around bathrooms and backup clothesthen finds out they’re severely anemic. The shock isn’t just the diagnosis. It’s realizing they adapted to something that deserved medical attention the whole time.
“I wasn’t taken seriously until I had proof on an ultrasound.”
Many people describe a frustrating loop: they report heavy bleeding and fatigue, they’re told to “try a different birth control,” and their symptoms are treated like an inconvenience instead of a health issue. Some say they were asked whether they were “sure” the bleeding was that bad, or told stress was the problem. For Black women in particular, that dismissal can feel familiaranother moment where pain is minimized. When imaging finally confirms fibroids, it’s validating… but also infuriating. People often wonder how different their options might have been if someone had ordered an ultrasound sooner.
“It wasn’t just bleeding. It was my whole life shrinking.”
Fibroids can quietly steal quality of life. Someone might stop exercising because bouncing hurts. They avoid long meetings because they need frequent bathroom breaks. They skip social events during their period because the bleeding is unpredictable. Dating and intimacy can become stressful if sex is painful or if body bloating makes them feel unlike themselves. What outsiders see as “a women’s issue” can actually affect work performance, mental health, relationships, and confidence. People often describe feeling trapped in a body that requires constant management.
“Every option felt like a trade-off.”
Another common theme is decision fatigue. Some people want to keep their uterus for fertility or personal reasons; others are done having children but still want choices that don’t feel extreme. People frequently describe being offered hysterectomy earlysometimes before hearing about medications, embolization, or ablation. Others go the opposite direction, trying medication after medication while anemia worsens. Many share that the best moment wasn’t choosing a specific treatmentit was finally meeting a clinician who explained options clearly, asked about life goals, and treated them as the expert on their own experience.
“Community helped me stop suffering in silence.”
Because fibroids can be stigmatized, many people feel isolated at first. But once they talk about it, they realize how many friends, coworkers, aunts, and cousins have similar stories. For Black women, that community connection can be powerfulespecially when it counters the “strong Black woman” pressure to endure pain quietly. People often describe a turning point when they started tracking symptoms, asking direct questions, seeking second opinions, and bringing someone with them to appointments for support. The common message is hopeful: you can’t always control fibroids, but you can control how much support you get while dealing with them.





