Table of Contents >> Show >> Hide
- Why COVID-19 Vaccines Still Matter in 2026
- What’s New for the 2025–2026 COVID-19 Vaccine Season
- COVID-19 Vaccine Schedule (2025–2026): The Practical Version
- Efficacy vs. Effectiveness: What the Numbers Really Mean
- Safety and Side Effects: What to Expect (and When to Call Someone)
- Getting Vaccinated Efficiently: The “Adulting” Checklist
- FAQ: Rapid-Fire Answers
- Conclusion: The Smart Way to Use COVID-19 Vaccines in 2026
- Real-World Experiences: What People Commonly Report (and What It Teaches Us)
If you’re wondering whether you “still need” a COVID-19 vaccine in 2025–2026, welcome to the club. The virus keeps evolving,
guidance keeps evolving, and your group chat keeps sending you screenshots with captions like “Wait, is this real??”
(Sometimes yes. Sometimes… absolutely not.)
This guide breaks down the current U.S. vaccine approach in plain American English: who it’s for, what the schedule looks like,
what “efficacy” really means in 2026, and how to think about your own risk without needing an advanced degree in Immunology
(or a strong relationship with your pharmacist, though that can help).
Quick note: This article is educational and not personal medical advice. If you have unique medical concerns (immunocompromised conditions, pregnancy, prior vaccine reactions), talk with a licensed clinician.
Why COVID-19 Vaccines Still Matter in 2026
The short version: vaccines remain one of the most reliable tools for reducing the risk of severe COVID-19especially
hospitalization and death. They’re not magical force fields (never were), and immunity fades over time (also never new).
But updated vaccines are designed to better match current strains and refresh protection when it’s worn thin.
What vaccines can (and can’t) do
- Best at: lowering the risk of severe illness, hospitalization, and death.
- Decent at: reducing symptomatic infection for a period of timeespecially soon after vaccination.
- Not perfect at: blocking every infection forever. Breakthrough infections happen, particularly as months pass and variants shift.
Think of it like a seatbelt: not a guarantee you’ll never get into a crash, but a major improvement in your odds if you do.
And unlike your car’s “check engine” light, vaccine updates are actually trying to help you.
What’s New for the 2025–2026 COVID-19 Vaccine Season
The big theme this season is individual-based decision-making (you might also hear “shared clinical decision-making”).
Translation: rather than a one-size-fits-all approach, the decision is meant to consider your age, health conditions, exposure risk,
and personal preferencesideally with a healthcare professional in the mix.
Which vaccines are available in the U.S.?
Three main options are available for 2025–2026 (depending on age):
- mRNA vaccines: Moderna and Pfizer-BioNTech
- Protein subunit vaccine: Novavax
Each works by teaching your immune system to recognize a key piece of the virus (the spike protein), so your body can respond faster
if you’re exposed later. They just use different “delivery styles” to get the lesson across.
What strains do the 2025–2026 vaccines target?
The 2025–2026 U.S. formulations are based on Omicron JN.1-lineage viruses. For this season, guidance indicates:
Moderna and Pfizer-BioNTech target LP.8.1, while Novavax targets JN.1. In real life, that means the vaccine
is trying to look more like what’s actually circulating, instead of shadowboxing last year’s variant.
COVID-19 Vaccine Schedule (2025–2026): The Practical Version
Vaccine schedules can look like a spreadsheet designed by a committee (because they are). Here’s the reader-friendly version.
Exact timing can depend on your previous doses, the product used, and immune status.
High-level schedule by age (typical scenarios)
| Age group | Typical 2025–2026 dose guidance | What that usually means |
|---|---|---|
| 6–23 months | Often 2 doses if unvaccinated; 1 dose if previously vaccinated | For many infants/toddlers starting fresh, it’s a short series; intervals commonly fall in the 4–8 week range. |
| 2–4 years | Typically 1 dose (Moderna) regardless of history | This age band is simplified compared with earlier seasons. |
| 5–11 years | Typically 1 dose | One updated dose is commonly used whether previously vaccinated or not. |
| 12–64 years | Typically 1 dose | Most people in this range receive a single updated dose; timing depends on last dose and product. |
| 65+ years | Typically 2 doses, spaced about 6 months apart (minimum intervals may apply) | Older adults are prioritized for longer-lasting protection through a two-dose seasonal approach. |
Timing rules you’ll hear a lot
- After your last COVID-19 vaccine: many schedules use a waiting period (often measured in weeks; some products use months).
- After a recent COVID-19 infection: you may choose to delay vaccination for about 3 months after symptom onset (or after a positive test if you had no symptoms).
- Mixing vaccine brands: it’s usually preferred to stay with the same product when recommended, but switching may be allowed in certain situations (availability, age transitions, etc.).
What if you’re pregnant, breastfeeding, or trying to conceive?
Pregnancy increases the risk of severe COVID-19 complications, and vaccination can be especially beneficial if you’re at higher risk.
Many clinicians and professional organizations continue to support vaccination during pregnancy and lactation, emphasizing informed,
individualized decision-making. If you’re pregnant (or planning to be), it’s worth a direct conversation with your OB-GYN or midwife.
What if you’re moderately or severely immunocompromised?
Immunocompromised people may need more than one 2025–2026 dose depending on vaccine history. For example, some guidance recommends two
2025–2026 doses after completion of an initial series, with revised intervals compared with the general population. Your clinician may also
tailor timing around treatments such as chemotherapy, organ transplant medications, or certain biologics.
Efficacy vs. Effectiveness: What the Numbers Really Mean
“Efficacy” usually refers to how well a vaccine performed in a controlled clinical trial. “Effectiveness” is how well it performs in
the real worldwhere people forget appointments, get exposed at weddings, and sometimes learn about “Daylight Saving Time” the hard way.
Why effectiveness changes over time
- Variants change: the virus evolves, and the match between vaccine and circulating strains can shift.
- Immunity wanes: protection tends to be strongest soon after vaccination and declines over months.
- Population differences: age, health conditions, and prior infection all influence outcomes.
What studies show (recent seasons)
Real-world studies from recent seasons consistently show that updated COVID-19 vaccines provide meaningful protection against severe outcomes,
particularly in older adults and higher-risk groups. For example, interim CDC network estimates for the 2024–2025 season found modest-to-moderate
protection against emergency/urgent care visits for adults and stronger protection against hospitalization in older adultsespecially soon after vaccination.
Pediatric analyses also found strong protection against emergency/urgent care visits during certain time windows after vaccination.
Bottom line: if your goal is avoiding a hospital stay, vaccination is still one of the best tools we haveespecially if you’re 65+,
immunocompromised, pregnant, or living with chronic conditions like diabetes, heart disease, lung disease, or kidney disease.
Safety and Side Effects: What to Expect (and When to Call Someone)
Most side effects are signs your immune system is practicing, not panicking. Common reactions usually show up within a day or two and fade quickly.
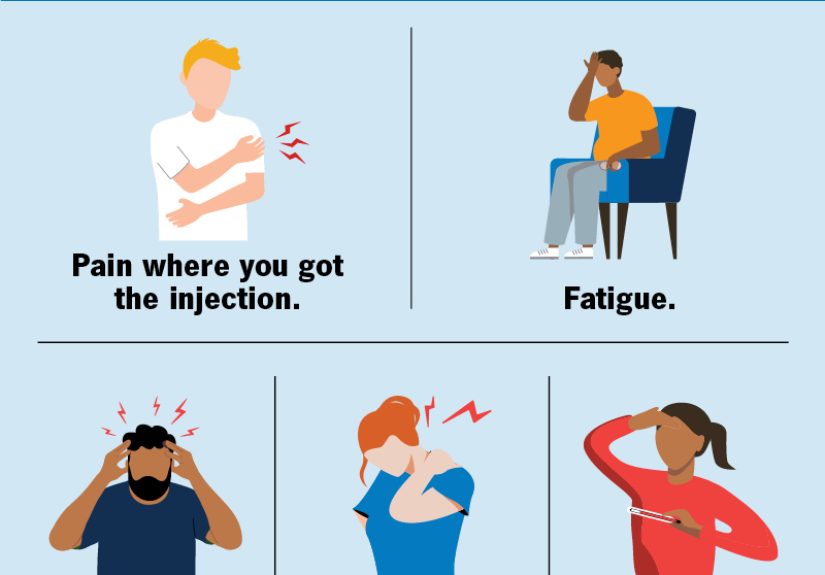
Common side effects
- Sore arm (classic)
- Fatigue
- Headache
- Muscle aches, chills, low-grade fever
- Swollen lymph nodes (especially near the arm where you got the shot)
Rare but important: myocarditis/pericarditis
Myocarditis and pericarditis have been observed rarely after mRNA COVID-19 vaccination, most often in adolescent and young adult males,
typically within about a week after vaccination. The overall risk is low, but it’s realwhich is why guidance sometimes discusses spacing doses
(for example, using longer intervals between first and second doses in multi-dose situations) to potentially reduce risk.
When to seek medical care
Get urgent medical attention if you develop chest pain, shortness of breath, a fast-beating/pounding heart, or faintingespecially within a week after vaccination.
Also seek help for any signs of a severe allergic reaction (hives, swelling of face/throat, trouble breathing).
Getting Vaccinated Efficiently: The “Adulting” Checklist
Can you get COVID-19 and flu shots at the same time?
In many cases, yes. COVID-19 vaccine can be given at the same visit as other vaccines, including influenza (and, when appropriate, RSV).
If you’re worried about feeling extra achy afterward, a practical tip is to use different arms and plan a lighter day afterwardlike you would after leg day.
What to bring (or remember)
- Your vaccine record (if you have it)
- A list of your medications and major health conditions
- Any history of vaccine reactions (especially myocarditis/pericarditis or severe allergy)
- A plan for the day after (hydration, rest, maybe not your most ambitious workout)
Examples: how different people might think about the decision
- A healthy 28-year-old remote worker: may decide to vaccinate to reduce time sick and lower risk of complications, especially before travel or a big work stretch.
- A 72-year-old with diabetes: usually has a strong case for vaccination, often with a two-dose seasonal approach to extend protection.
- A parent of a 3-year-old: may talk with the pediatrician about timing, especially if the child recently had COVID-19 or has asthma.
- A person on immune-suppressing meds: may need a tailored plan for dose number and timing around treatment.
FAQ: Rapid-Fire Answers
“I already had COVID. Doesn’t that count?”
Prior infection can provide some protection, but it also fades. Vaccination after infection can broaden and refresh immune response. Many people choose to
wait around three months after infection before getting an updated dose.
“Which vaccine is best?”
There’s generally no single “best” for everyone. The best vaccine is the one that’s age-appropriate, available, and fits your medical situation.
If you have a history of reactions or specific concerns, your clinician can help choose among options.
“Will the vaccine prevent Long COVID?”
Evidence suggests vaccination can reduce the risk of Long COVID by lowering the odds of infection and severe illness, but it doesn’t eliminate risk entirely.
The cleanest strategy is layered protection: vaccination + staying home when sick + good ventilation when possible.
Conclusion: The Smart Way to Use COVID-19 Vaccines in 2026
The most realistic, evidence-based view is this: COVID-19 vaccines are a risk-reduction tool. They’re especially valuable for people 65+,
pregnant people, immunocompromised individuals, and anyone with medical conditions that raise the chance of severe disease.
For others, the decision can be more individualizedbased on your health, exposure risk, and how badly you want to avoid being flattened for a week
right before a wedding, deadline, vacation, or your kid’s school play.
If you’re unsure, use the simplest decision framework:
What’s my risk of severe COVIDand how much do I value reducing it?
Then talk it through with a clinician who knows your history. Your immune system can handle the workout. Your calendar will thank you.
Real-World Experiences: What People Commonly Report (and What It Teaches Us)
Numbers are essential, but experiences are often what make vaccine decisions feel real. Across clinics, pharmacies, and family dinner tables,
a few patterns come up again and againespecially in a season where guidance emphasizes individual decision-making.
1) “The side effects were annoying, but predictable.”
A lot of people describe the post-shot day as “a forced nap with a sore arm.” They’ll feel tired, a bit achy, maybe slightly feverish,
and then they bounce back. The practical lesson is planning: don’t schedule your vaccine 12 hours before a red-eye flight, a big presentation,
or the day you promised to help a friend move a couch up three flights of stairs. People who have the smoothest experience often do two simple things:
hydrate, and give themselves permission to take it easy the next day.
2) “It didn’t stop me from getting COVID, but it changed the outcome.”
This is one of the most common narrativesespecially among older adults and people with chronic conditions. Someone gets vaccinated, later catches COVID,
and still gets sick… but avoids the ER or hospitalization. They’ll say things like, “I felt rough for a few days, but it never got scary.”
While personal stories aren’t scientific proof, they do align with what effectiveness studies have repeatedly shown: vaccines tend to provide their strongest
benefit against severe disease. People also mention shorter illness duration or faster return to normal routines, which matters in the real world
where “missing a week of work” can ripple into everything.
3) “Decision-making feels harder now, so people want clear risk categories.”
When recommendations shift toward individualized choices, people naturally ask, “Okay… so which bucket am I in?” In real conversations,
clinicians often translate risk into plain language: age 65+, pregnancy, immunocompromised conditions, chronic heart/lung/kidney disease, diabetes,
and living in long-term care are common “higher benefit” categories. People who live with or care for high-risk relatives also often choose vaccination
because they’re thinking beyond themselvesreducing the chance of bringing infection home, or reducing severity if they get sick.
4) “Parents want reassurance, not pressure.”
Parents frequently report that what they want most is a calm, non-judgmental discussion. They ask about timing after a recent infection,
whether their child’s asthma changes the equation, and how to weigh side effects against benefits. Pediatric visits that go well tend to include:
(a) a clear summary of what the schedule typically looks like for the child’s age, (b) an honest explanation that protection wanes, and
(c) a reminder that the goal is usually preventing severe outcomes rather than guaranteeing zero infections.
5) “People love convenienceso co-administering vaccines helps.”
A surprisingly powerful experience is simply getting multiple vaccinations in one visit. Many people report that bundling flu + COVID-19 (and, for some,
RSV) feels like “one errand instead of three,” which increases follow-through. Some choose separate arms or separate days because they prefer to minimize
feeling wiped out. Both approaches can be reasonable; the key is reducing barriers so people actually get the protection they intend to get.
Taken together, these experiences point to a common theme: vaccine decisions get easier when people have (1) realistic expectations, (2) a plan for timing,
and (3) a risk-based explanation that respects their situation. In other words: clear info, zero drama, and maybe a snack afterward.